
Vol 2 | Issue 1 | Jan – June 2017 | Page 49-51 | Vivek Pandey, Sandesh Madi, Naveen Mathai
Authors: Vivek Pandey [1], Sandesh Madi [1], Naveen Mathai [1].
[1] Kasturba Medical College, Manipal University, Karnataka, India- 576104
Address of Correspondence
Dr. Vivek pandey
Kasturba Medical College, Manipal University,
Karnataka, India- 576104
Email: vivekortho@gmail.com
1. Slow or accelerated Rehabilitation after cuff repair, A matter of time or is it?
There exists lot of ambiguity in rehabilitation protocols among shoulder surgeons following arthroscopic rotator cuff repairs. It is an overwhelming task to balance between initiating early range of motion without disturbing the integrity of the cuff repair. Following arthroscopic single-tendon rotator cuff repair, Mazzocca et al [1] revealed that no differences in quality of life scores or rotator cuff healing were identified after comparing two groups of patients undergoing either immediate (within three days) or delayed (after twenty eight days) postoperative rehabilitation protocols. Other factors such as age of the patient, cuff and bone quality, tear geometry, repair techniques and implants play vital role in determining the rehabilitation regime and probably needs to be tailored accordingly. Moreover, recent meta-analysis by Chang et al [2] comparing early versus delayed mobilisation protocols revealed hardly any differences in rotator cuff healing, final shoulder range of motion or patient outcomes.
2. Massive cuff tears: approaches for a costly affair
Presently, there are three possible strategies for the management of massive cuff tears with pseudopalsy without Osteoarthritis: 1) Arthroscopic Rotator Cuff Repair (ARCR) with option to arthroscopically revise once. 2) ARCR with immediate conversion to Reverse Total Shoulder Arthroplasty (RTSA) on potential failure, or 3) Primary RTSA. In an economic and decision based analysis (Markov decision model), Dornan et al have concluded that Primary ARCR with conversion to RTSA on potential failure was found to be the most cost-effective strategy in such cases [3]. An important observation was this result independent of age of the patient. Primary ARCR with revision ARCR on potential failure was a less cost-effective strategy. RTSA is not the panacea for massive cuff tear management and should be offered only as a last resort after exhausting available repair options.
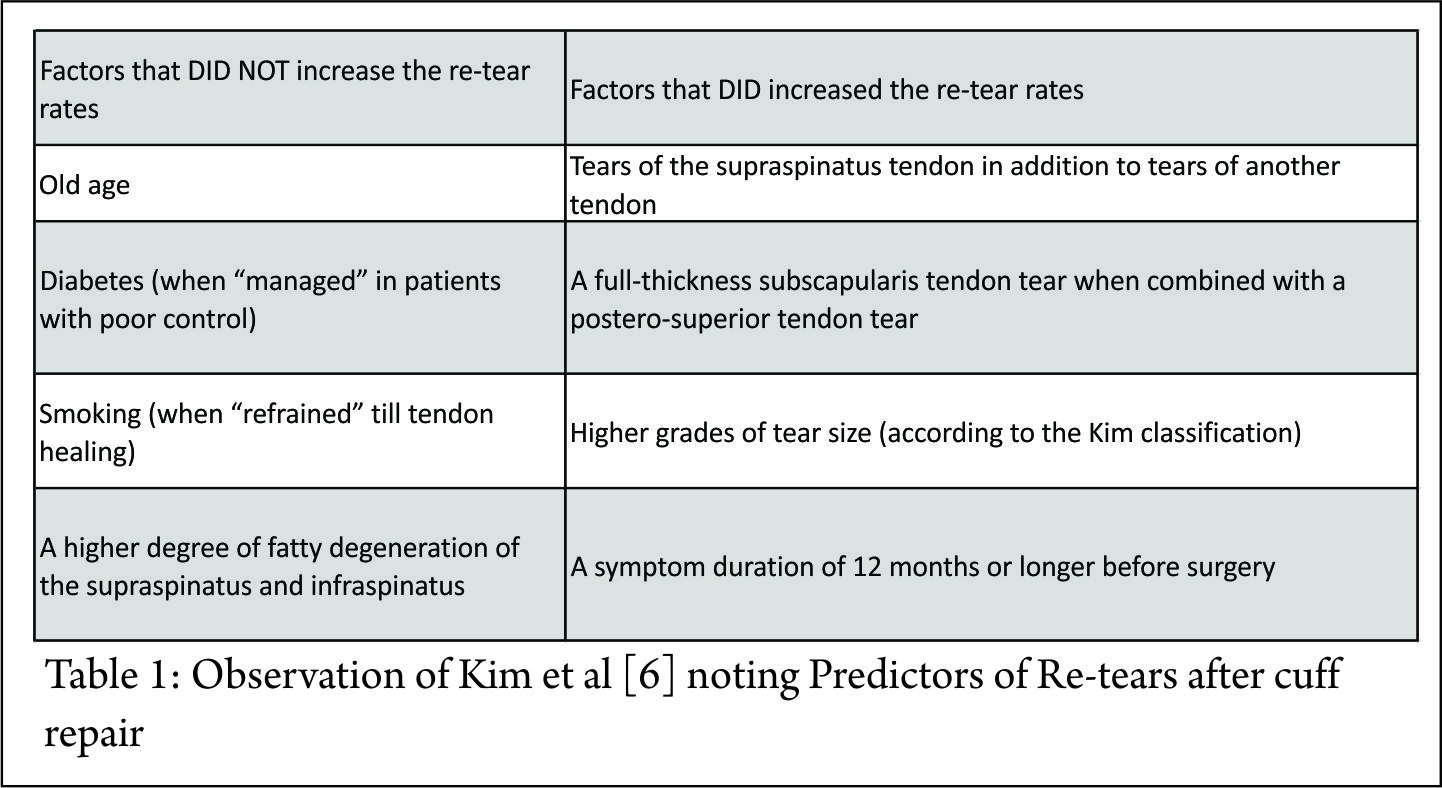
3. Predictors of Re-tears after cuff reapir
There are diverse factors that determine the healing of repaired rotator cuff tears. Reported rates of re-tear after rotator cuff repair widely varies from 11% to 94% [4,5] . In a prognostic case series, Kim et al [6] attempted to identify pre-operative factors that can predict the rate of re-tears following rotator cuff repairs. The observations made are noted in table 1 and included mostly the charaterictic of the tear and duration of symptoms. Surprisingly comorbidities like old age, diabetes, smoking and fatty degeneration of tendons did not significantly predict re-tears.
4. Does the repair of cuff stays for long?
A Long term outcome after rotator cuff repair, 2-10 year long study. After the repair of the rotator cuff, it has always been intriguing that what happens to the repair in long term? Does the repair remains intact long enough and does the clinical results do not deteriorate over time? Heuberer et al [7] published their short and long term data recently involving arthroscopic repair of full thickness supraspinatus tear with/without partial infraspinatus tear. They followed 30 patients at 2- and 10 year with clinical scores ((Constant Murley and UCLA) and MRI for structural healing. MRI at two year follow up revealed 42% of patients with a full-thickness re-rupture, while 25% had a partial re-rupture, and 33% of tendons remained intact. The 10-year MRI follow-up (129 ± 11 months) showed 50% with a total re-rupture, while the other half of the tendons were partially re-ruptured (25%) or intact (25%). The UCLA and constant score remained high at 2- and 10 year follow up as compared to preop status. The constant total score and strength subscore remained high in patients with intact tendon versus those with retear. Majority patients (83.3%) rated their satisfaction as excellent. However the complete retear rates are almst 50% with single row. It would be interesting to analyse the repair of similar tears with double row and look at the outcome.
5. What is the critical Glenoid bone loss after which soft tissue bankart repair does not restore glenohumeral biomechanics and movement?
It was Itoi et al who brought the concept of critical bone loss of 21% in glenoid beyond which a soft tissue Bankart repair may not suffice to provide stability [8]. This brought the concept of bone augmentation using Latarjet procedure, Iliac crest graft or distal tibia allograft. However, recently Shin et al [9] challenged this concept of reconsidering this 21% bone loss as critical limit. In their study on eight cadaveric shoulder, they created 10%, 15%, 20% and 25% anteroposterior glenoid bone loss. After the soft tissue Bankart repair, the shoulder were subjected to range of motion, translation and humeral head position at 600 abduction with 40N rotator cuff muscle loading. They concluded that critical bone loss after which the biomechanics of the shoulder cannot be restored is 15%, and not 20-25% which has been the current recommendation for bone augmentation.
6. RSA versus conservative treatment in 3- or 4-part fracture of proximal humerus in elderly. Which is better?
Since the advent of RSA and its expanding indication, there has been a debate about the use of RSA in the treatment of proximal humeral fracture especially elderly patients. ORIF and hemiarthroplasty (HA) remained two essential form of treatment in these patients. However, ORIF carried a higher complications like implant failure due to osteoporosis and comminution whereas HA caused problem due to tuberosity nonunion. Hence, RSA became increasingly a popular option for the treatment of such challenging fracture. However, Roberson et al [10] did a two year retrospective review of patients older patients (>70 year) who underwent RSA for 3- or 4-part fracture of proximal humerus versus conservative treatment. They reported minimal benefits of RSA over conservative treatment at two years. The RSA group was no better than conservative group whether it was achievement of range of movement or patient reported outcomes.
7. Can local application of Vancomycin powder reduce the infection rate after total shoulder replacement?
Despite all the aseptic measures, the Methicillin resistant and Propionibacterium infection after the total shoulder replacement is a nightmare for the surgeon. The cost to treat postoperative infection till revision can range up 47260$ in USA. Any measure which can reduce the infection rate and cost to treat such problem will be a great idea. Based upon prevalent rates of infection in shoulder arthroplasty, Daniel Hatch et al [11] did an analysis of cost effective of local use of Vancomycin powder (2-18$/1000 mg) usage over the local wound to prevent such infection, and concluded that local application of Vancomycin powder is going to be highly cost effective in preventing such infection.
References
1. Mazzocca AD, Arciero RA, Shea KP, Apostolakos JM, Solovyova O, Gomlinski G et al. The effect of early range of motion on quality of life, clinical outcome, and repair integrity after arthroscopic rotator cuff repair. Arthroscopy. 2017 Jun; 33(6):1138-1148.
2. Chang K, Hung C, Han D, Chen W, Wang T, Chien K. Early versus delayed passive range of motion exercise for arthroscopic rotator cuff repair: A meta-analysis of randomized controlled trials. Am J Sports Med 2014; 43: 1262-1273.
3. Dornan GJ, Katthagen JC, Tahal DS, Petri M, Greenspoon JA, Denard PJ et al. Cost-Effectiveness of Arthroscopic Rotator Cuff Repair Versus Reverse Total Shoulder Arthroplasty for the Treatment of Massive Rotator Cuff Tears in Patients With Pseudoparalysis and Nonarthritic Shoulders. Arthroscopy. 2017 Apr 30; 33(4):716-25.
4.Le BT, Wu XL, Lam PH, Murrell GA. Factors predicting rotator cuff retears: An analysis of 1000 consecutive rotator cuff repairs. Am J Sports Med 2014; 42: 1134-1142.
5.Wang VM, Wang FC, McNickle AG, et al. Medial versus lateral supraspinatus tendon properties: Implications for double-row rotator cuff repair. Am J Sports Med 2010; 38: 2456-2463.
6. Kim IB, Kim MW. Risk factors for retear after arthroscopic repair of full-thickness rotator cuff tears using the suture bridge technique: Classification system. Arthroscopy. 2016. Nov 30;32(11):2191-200.
7. Heuberer PR, Smolen D, Pauzenberger L, Plachel F, Salem S, Laky B, Kriegleder B, Anderl W. Longitudinal Longterm Magnetic Resonance Imaging and Clinical Follow-up After Single-RowArthroscopic Rotator Cuff Repair: Clinical Superiority of Structural Tendon Integrity. Am J Sports Med. 2017 May;45(6):1283-1288
8. Itoi E, Lee SB, Berglund LJ, Berge LL, An KN. The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: a cadaveric study. J Bone Joint Surg Am. 2000 Jan;82(1):35-46
9. Shin SJ, Koh YW, Bui C, Jeong WK, Akeda M, Cho NS, McGarry MH, Lee TQ. What Is the Critical Value of Glenoid Bone Loss at Which Soft Tissue Bankart Repair Does Not Restore Glenohumeral Translation, Restricts Range of Motion, and Leads to Abnormal HumeralHead Position? Am J Sports Med. 2016 Nov;44(11):2784-2791.
10. Troy A. Roberson, Charles M. Granade, Quinn Hunt, James T. Griscom, Kyle J. Adams, Amit M. Momaya, Adam Kwapisz, Michael J. Kissenberth, Stefan J. Tolan, Richard J. Hawkins, John M. Tokish. Nonoperative management versus reverse shoulder arthroplasty for treatment of 3- and 4-part proximal humeral fractures in older adults. Journal of Shoulder and Elbow Surgery, 2017-06-01, Volume 26, Issue 6, Pages 1017-1022,
11. The cost-effectiveness of vancomycin for preventing infections following shoulder arthroplasty: a break even analysis. M. Daniel Hatch, Stephen D. Daniels, Kimberly M. Glerum, Laurence D. Higgins. Journal of Shoulder and Elbow Surgery, 2017-05-01, Volume 26, Issue 5, Pages e144-e145
| How to Cite this article: Pandey V, Madi S, Mathai N. Potpourri – Recent and relevant literature in Shoulder Arthroplasty, Arthroscopy and Trauma . Journal of Clinical Orthopaedics Jan – June 2017; 2(1):49-51. |