
Vol 2 | Issue 1 | Jan – June 2017 | Page 10-13 | Ashok Rajgopal, Vivek Dahiya
Authors: Ashok Rajgopal [1], Vivek Dahiya [1].
[1] Fortis Bone & Joint Institute. Fortis Group of Hospitals, Delhi, NCR
Address of Correspondence
Dr. Ashok Rajgopal
.
Email: a_rajgopal@hotmail.com
Abstract
Introduction: Total knee replacement is a Gold standard for treatment of arthritis of knees. It has stood the test of time and has delivered excellent results. With time the number of knee replacement are increasing and the age of patients are decreasing. Technological advances have kept pace with the newer designs which have helped deliver better results to the patients.
Key Words: Total knee replacement, new updates, technology.
Background
The knee is the largest joint of the human body and it is involved in almost all the activities of daily living. It is prone to repetitive micro trauma leading to wear and tear of the cartilage which in turn leads to osteoarthritis of the knee joint. Osteoarthritis makes a knee stiff, painful to walk on and inhibits an individual from performing activities of daily living. Exercises, physiotherapy and over the counter pain killers do help initially but with time it becomes imperative to think about knee replacement. Total knee replacement is the gold standard for treatment of knee arthritis and has shown predictably excellent results over the past 20 years [1,2]. In recent times due to increased awareness more and more patients are opting for this surgery not only to maintain but also to improve their quality of life. The patients hope to participate in all the activities and be physically active. They don’t want to adhere to the age old nuances of “Let it be , you are getting old”. In the past two decades the average age of the patients undergoing knee replacement surgery has come down resulting in an increased demand on the knee joint [3]. The challenges for the Orthopaedics surgeon are manifold. Not only does he need to correct the deformity, and enable the patient to get back to a normal life but also think about life of the prosthesis. This increased demand has forced the surgeons to deliberate and research extensively in order to overcome the drawbacks of the older conventional knee systems and also meet the challenges faced by them in their daily surgical practice.
Advances in the past two decades have been able to give the surgeons the tools to satisfy their patients over the whole spectrum. In this article we shall try to enumerate the recent advances in total knee replacement and how they help the patients.
As we know in 1860, Verneuil proposed interposition arthroplasty, involving the insertion of soft tissue to reconstruct the joint surface. Since then, pig bladder, nylon, femoral sheath, anterior bursa of the knee, cellophane, and many other materials have been used, but results were disappointing. The use of metallic interposition arthroplasty began in the late 1930s. Today implants are made of a highly polished cobalt chrome alloy which is a very strong alloy well tolerated and accepted by the human body. Zirconium implants (Fig.1) offer another bearing surface akin to ceramics with a very low coefficient of friction. The long term results of these implants are awaited and we shall then know if it is worth the high price [4]. The polyethylene insert which is placed between the two metal components is highly cross linked which prevents its wear and tear. Sterilization methods have helped reduce the wear and tear rate of the insert. Gamma sterilization in the past led to early catastrophic wear and breakdown of the insert. Now a days EtO sterilization has solved the problem. Addition of vitamin E in the substance of the insert is said to delay its degradation [5,6].
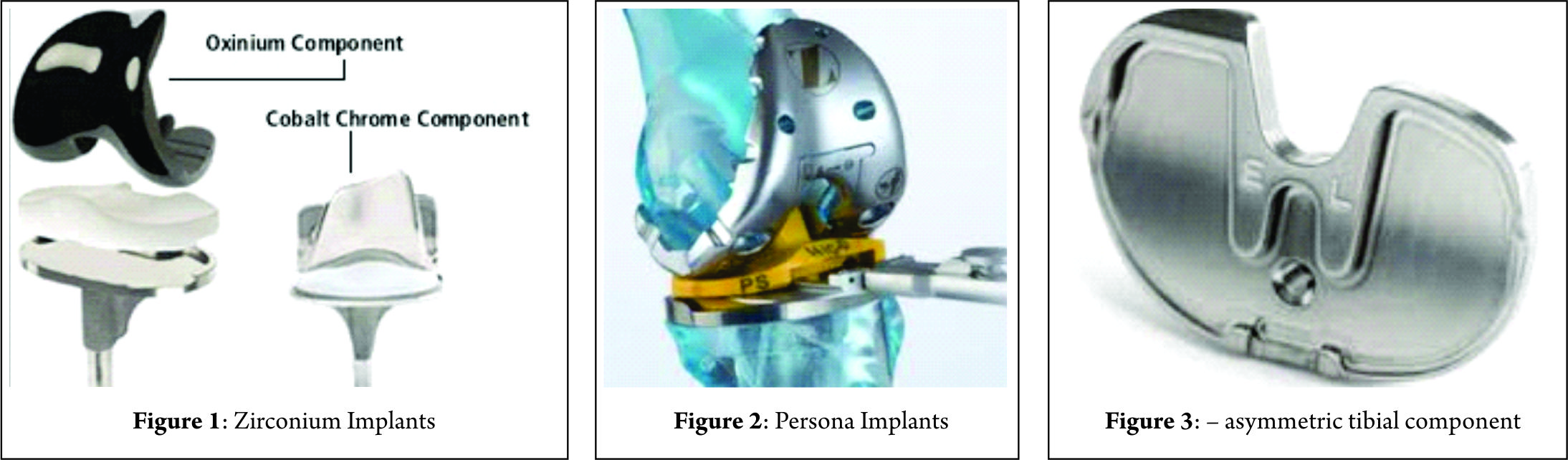
Design of the knee implant has a bearing on the result of the surgery-both in the survivorship of the implant and in terms of patient satisfaction. The knee joint has three bones that articulate with each other. For the implant to be successful the components have to be well synchronised with each other and also perform their own functions independently. The femoral component (part of the lower thigh forming the knee) should be well fitting on the host bone, and should not over hang the bone otherwise it will rub with the soft tissues causing pain. It should also provide a good and friendly surface for the knee cap (patella) to glide on. Modern designs take care of this aspect. The Persona implant (Fig. 2) from Zimmer has femoral components in 2 mm increments and each size comes with a standard and a narrow option. The number of sizes available are in 2 mm increments in both planes,a design which helps in providing a better fit of the implant. No two individuals are alike so why should two knees be the same? To facilitate this there are several permutations and combinations available to the surgeon which provide for the ideal fit. The Persona implant is also the most patella friendly implant available. This allows for ease of gliding of the patella on the femoral component helping to achieve a better and more efficient thigh muscle function. This in turn leads to better knee joint range of motion and gait pattern.
The Tibial component (part of the leg bone which participates in the knee) is also an important part of the knee. Traditionally they were made symmetric whereas the normal human anatomy is asymmetric [7].(Fig.3) What this means that the shape of the tibial component should closely approximate the original anatomy of the bone. In the Persona Knee system the tibial component comes in 9 sizes with 1mm increments again allowing the surgeon much more flexibility in choosing the exact size of the implant for the patient. As with the femoral component overhang is going to rub against the soft tissues and cause pain [8]. The question as to resurface the patella or to leave it alone is eternal. The proponents of either are numerous but so far no consensus has been formed [9]. So has been the case for posterior cruciate ligament retention or substitution. All implants are available in cruciate retaining and posterior stabilized designs.

Newer metals like Trabecular metal have in fact revolutionized the area of knee replacement. These metals are extremely porous and have elasticity of modulus approximating that of natural bone. The porosity allows for growth of bone into the implant(Fig.4). This helps in better integration of the implant to the bone and thus increasing the life of the implant [10,11]. Also there is no need to use bone cement to fix these implants to bone. It has found use in revision surgery of the knee too. Revision surgery is needed when the original total knee replacement fails and a new surgery is needed to address all the myriad issues where trabecular metal cones are helpful to reconstruct the lost bone. They are used to build up the defect in bones and allow for the host bone to grow into them to achieve a more biological end result.
Computer assisted surgery has been in use for a long time. Earlier devices were large in size (Brain Lab) and cumbersome to useresulting in an increase in surgery time. Newer devices are gravitating towards hand held devices such as the iASSIST (Zimmer)(Fig 5) or eNdtrac (Stryker)(Fig 6). These are surgical guidance systems engineered to improve the accuracy and alignment of total knee replacement surgery. They are also less invasive and more surgeon friendly. Once the learning curve is over there is hardly any change in surgery time as compared to before12. Among these devices is the Navio (Fig. 7) system from Smith & Nephew. It allows for intraoperative navigation and then the use of a handheld robot to perform the cuts of the bone. At present available only for the unicompartmental knee. The software for the total knee replacement is to be released soon.
Customized knee implants wherein the implant is designed for the patient after pre-operative imaging is also being used in the USA. Conformist manufactures these implants. Individualized fit and bone conservation are their hallmarks. These unfortunately are not available in India yet [13].
Awareness is leading to younger patients opting for knee surgery. Every knee arthritis does not need a total knee replacement. In case only one compartment is involved then only that part can be replaced. This is called unicompartmental knee replacement. Unicompartmental knee replacement is getting to be more widely used than before and is well accepted. It is a smaller procedure, allows the patient to recover faster and gives a more natural feel of the knee. It also allows the patient to continue with a fairly aggressive life style.

Blood loss following surgery is expected, but the quantity of blood loss leads to several problems [14]. Constant endeavours to lessen the blood loss are underway. Use of tranexamic acid perioperatively has helped reduce the blood loss after total knee replacement. It is being used both intravenously and by injecting into the tissues around the surgical site15. Autologous blood transfusion is also a way to deal with the dangers of blood transfusion. It allows for the patient to receive their own blood which was given 3 to 6 weeks prior to surgery.
Use of technology is increasing in this field. Navigation and customized implants are at one end of the spectrum. The other end is occupied by Big Data. The immense amount of data and surgeon experience that is available all around is being understood now. It will be used to fabricate protocols to increase the surgeons and hospitals efficiency while dealing with total knee replacement patients. Big data combined with the joint registries will help the surgeons to make an informed choice on their choice of implants, surgical techniques, pain management protocols and postoperative rehabilitation.
Experience and hospital management systems have helped us evolve faster rehabilitation programs. They consist of patient education prior to surgery, ultrasound guided nerve blocks to reduce the intensity of post-operative pain, earlier and more aggressive rehabilitation and earlier discharge from the hospital. Patient education makes the patient more aware of the procedure and their expectations. They learn about the normal course of recovery and hence are more involved in the whole process. The commonest cause for delay of surgery is the fear of pain. Once the anesthesia wears off the patients will have some pain. Analgesics be it non opiodal or opiods have their limitations. Increased pain aggravates the co- morbidities and less rehabilitation. Ultrasound guided nerve blocks and placement of femoral nerve catheters does help a long way to reduce the pain [16,17]. So does the ”Ipac”, which involves instillation of an analgesic cocktail in the posterior capsule and the surgical field anteriorly. Early rehabilitation and mobilization helps reduce the incidence of DVT and PE, allows for earlier patient confidence in walking and leads to an early recovery. All these contribute to making the whole process more patient friendly and efficient for the hospitals to manage.
These advances have helped surgeons to satisfy their patients and have allowed the patients to achieve their goals and expectations to a large extent.
References
1. Twenty-Five-Years and Greater, Results After Non modular cemented Total Knee Arthroplasty. Ritter MA, Keating EM, Sueyoshi T, Davis KE, Barrington JW, Emerson RH.1. Twenty-Five-Years and Greater, Results After Non modular cemented Total Knee Arthroplasty. Ritter MA, Keating EM, Sueyoshi T, Davis KE, Barrington JW, Emerson RH.J Arthroplasty. 2016 Oct;31(10):2199-202. doi: 10.1016/j.arth.2016.01.043. Epub 2016 Feb 4.2. How do knee implants perform past the second decade? Nineteen- to 25-year followup of the Press-fit Condylar design TKA.Patil S, McCauley JC, Pulido P, Colwell CW Jr.ClinOrthopRelat Res. 2015 Jan;473(1):135-40.3. Total knee replacement in young, active patients: long-term follow-up and functional outcome: a concise follow-up of a previous report.Long WJ, Bryce CD, Hollenbeak CS, Benner RW, Scott WN.J Bone Joint Surg Am. 2014 Sep 17;96(18)4. Twelve-Year Outcomes of an Oxinium Total Knee Replacement Compared with the Same Cobalt-Chromium Design: An Analysis of 17,577 Prostheses from the Australian Orthopaedic Association National Joint Replacement Registry.Vertullo CJ, Lewis PL, Graves S, Kelly L, Lorimer M, Myers P.J Bone Joint Surg Am. 2017 Feb 15;99(4):275-283. 5. Contribution of Surface Polishing and Sterilization Method to Backside Wear in Total Knee Arthroplasty.Teeter MG, Lanting BA, Shrestha KR, Howard JL, Vasarhelyi EM.J Arthroplasty. 2015 Dec;30(12):2320-2.6. The influence of sterilization method on articular surface damage of retrieved cruciate-retaining tibial inserts. Greulich MT, Roy ME, Whiteside LA.J Arthroplasty. 2012 Jun;27(6):1085-93. 7. How Much Does the Anatomical Tibial Component Improve the Bony Coverage in Total Knee Arthroplasty ? Jin C, Song EK, Prakash J, Kim SK, Chan CK, Seon JK. J Arthroplasty .2017 Jun; 32(6):1829-18338. Gait Parameters and Functional Outcomes After Total Knee arthroplasty Using Persona Knee System With Cruciate Retaining and Ultracongruent Knee Inserts. Rajgopal A, Aggarwal K, Khurana A, Rao A, Vasdev A, Pandit H. J. Arthroplasty. 2017 Jan ;32(1):87-919. Is Selectively Not Resurfacing the Patella an Acceptable Practice in Primary Total Knee Arthroplasty?Maradit-Kremers H, Haque OJ, Kremers WK, Berry DJ, Lewallen DG, Trousdale RT, Sierra RJ.J Arthroplasty. 2017 Apr;32(4):1143-1147. 10. Trabecular metal tibial knee component still stable at 10 years.Henricson A, Nilsson KG. Acta Orthop. 2016 Oct ;87(5) : 504-1011. Mid-term results of total knee arthroplasty with a porous tantalum monoblock tibial component.Hayakawa K, Date H, Tsujimura S, Nojiri S, Yamada H, Nakagawa K. Knee. 2014 Jan;21(1):199-203. 12. Total knee arthroplasty with computer-assisted navigation more closely replicates normal kneebiomechanics than conventional surgery.McClelland JA, Webster KE, Ramteke AA, Feller JA.Knee. 2017 Jun;24(3):651-656. 13. Evolution of customization design for total knee arthroplasty.Slamin J, Parsley B. Curr Rev Musculoskelet Med. 2012 Dec;5(4):290-5. 14. Enhanced recovery protocol and hidden blood loss in patients undergoing total knee arthroplasty.Dhawan R, Rajgor H, Yarlagadda R, John J, Graham NM. Indian J Orthop. 2017 Mar-Apr;51(2):182-18615. Effect of Tranexamic Acid on Transfusion Rates Following Total Joint Arthroplasty: A Cost and Comparative Effectiveness Analysis.Evangelista PJ, Aversano MW, Koli E, Hutzler L, Inneh I, Bosco J, Iorio R.OrthopClin North Am. 2017 Apr;48(2):109-115.16. Does Addition of Adductor Canal Blockade to Multimodal Periarticular Analgesia Improve Discharge Status, Pain Levels, Opioid Use, and Length of Stay after Total Knee Arthroplasty? Gwam CU, Mistry JB, Richards IV, Patel D, Patel NG, Thomas M, Adamu H, Delanois RE. J Knee Surg. 2017 May 2. 17. Multimodal infiltration of local anaesthetic in total knee arthroplasty; is posterior capsular infiltration worth the risk? a prospective, double-blind, randomised controlled trial. Pinsornsak P, Nangnual S, Boontanapibul K.Bone Joint J. 2017 Apr;99-B(4):483-488. .
| How to Cite this article: Rajgopal A, Dahiya V. What is New in Total Knee Replacement. Journal of Clinical Orthopaedics Jan – June 2017; 2(1): 10-13. |